Progress Notes, or clinical record-keeping, is a key aspect of professional practice and delivery in health and social care. Properly documenting Progress Notes using best practice procedures is important as they should enhance communication between various healthcare professionals and enable the continuity of care. Furthermore, when it comes to auditing the quality of care services being provided or investigating any wrongdoing or complaints, these records are often the first thing regulatory bodies refer to.
Poor record-keeping can increase legal risks, jeopardize care, prolong hospital admissions, lead to unnecessary and repeated tests, and increase the risk of misdiagnosis. Therefore, it is vital for healthcare professionals to review what needs to be recorded and how.
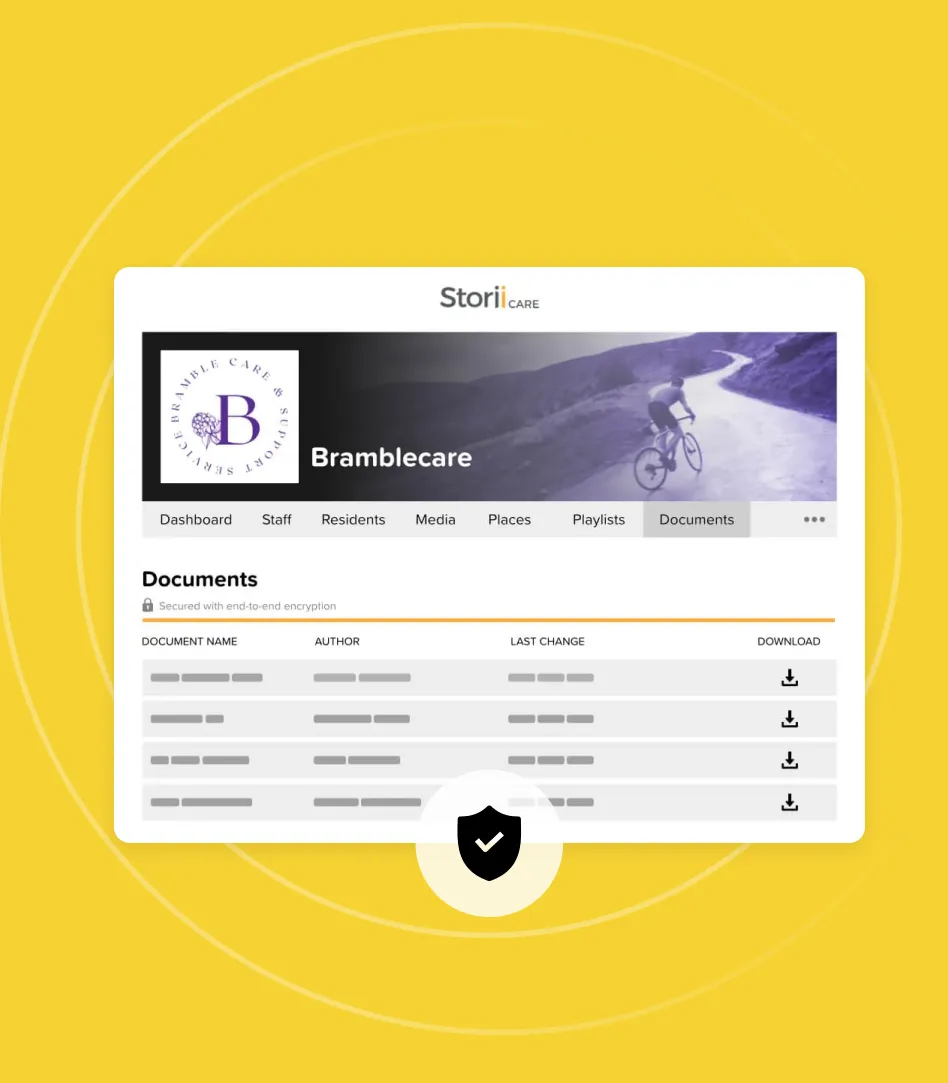
Why You Should Consider Going Digital
Hand-written, paper Progress Notes have been the standard in healthcare up until now. Technology is beginning to replace this practice and there are benefits to that. For example, documentation is widely believed to contribute to care staff burnout and it takes significant time that would be better spent with residents or service users. Digital care management systems lift the burden on providers by:
- Making notes clear and quick to read
- Pinpointing key information with rich text options
- Reducing incidents or missing information
- Embedding best-practice guidance
- Reducing time spent on record-keeping
- Making it easy to search for a specific entry
What Should be in a Progress Note
The following should be documented in Progress Notes:
- The note ‘type’ (i.e. service being recorded)
- What occurred during the date/times specified
- What support was offered and by whom
- A service user’s progress towards a goal identified in their care plan (actions taken, barriers identified)
- How the individual’s needs are being met
- Any noticeable changes to the Service User’s mood or engagement
- Any new needs that have been identified
- Any positive or negative findings from appointments, exams, tests, etc.
- All communication or attempts to contact other health services or relatives involved with the Service User (phone calls, emails, faces, in-person conversation)
- Referrals made
- Written/verbal instructions and/or educational materials given to the Service User
- All informed consent decisions
- Treatment details and future treatment recommendations
- Any incidents of noncompliance or objections to care/case management
- References to the previous note recorded if applicable
What Should Not be in a Progress Note
Progress Notes should NOT:
- Use abbreviations that wouldn’t be immediately recognized by the general public (for example, CD could mean ‘chemical dependency’ or ‘Chron’s Disease’)
- Include casual, offensive, or personal comments (observations and objective statements only)
- Be altered in a way that is untraceable
- Include assumptions (i.e. A diagnosis that is not on their record. For example, writing: ‘Ruth appears to be suffering from anxiety’ instead of ‘Ruth is displaying symptoms consistent with anxiety; increased heart rate, sweating, loss of appetite’)
- Contain opinions or impressions, unless you are clearly stating that it is your own
Examples of Proper Documentation
Good clinical documentation objectively states what happened and what you observed when interacting with the individual in care. It is detailed and accounts for all important information that may need to be referred to or follow up on. As the old adage goes, “If you didn’t get it in writing, it didn’t happen.”
Here are a few examples to show you the contrast between ideal Progress Notes and poor Progress Notes:
“Went to get Mable ready for bed and she was absolutely volatile. Screaming, hitting, kicking. I told her I would come back when she’d calmed down.”
Vs.
“I went in to get Mable ready for bed at 7 pm. When I attempted to help her out of the recliner to get her nightgown on, she smacked my arm, began kicking her feet and yelled at me to leave. I told her that I didn’t mean to upset her. I’d give her a few more minutes and would be back at 7:15 to start her routine.”
“John said he called and made an appointment with Dr. Carter (gastrointerologist) for Wednesday, April 5 at 10:30 am. This is in regards to the lower, left quadrant abdominal pain he’s been experiencing since last week.”
Vs.
“John still having abd pain. Appt with GI Wednesday.”
“Mercy Hospital contacted at 12:43 pm. They informed us that Sue is discharging to Methodist East in the morning. Methodist East contacted and spoke to Clayton on 8 North Ward. He informed me that Sue is waiting for renal stone removal. She will likely have this procedure on December 11 or 12. She is in good spirits. I faxed her drug chart to Mercy this morning. Sue’s husband came by around 2 pm and collected some things for her. Will follow up with Dr. Carter re: post-op treatment.”
Vs.
“Mercy called and said Sue is discharging to Methodist East in the am. Waiting on renal stone removal. Appears to be in good spirits. Faxed her rx chart to Mercy and gave her things to Dale. Will contact Dr. Carter tomorrow."

%2011.50.25.png)
%2011.50.48.png)